


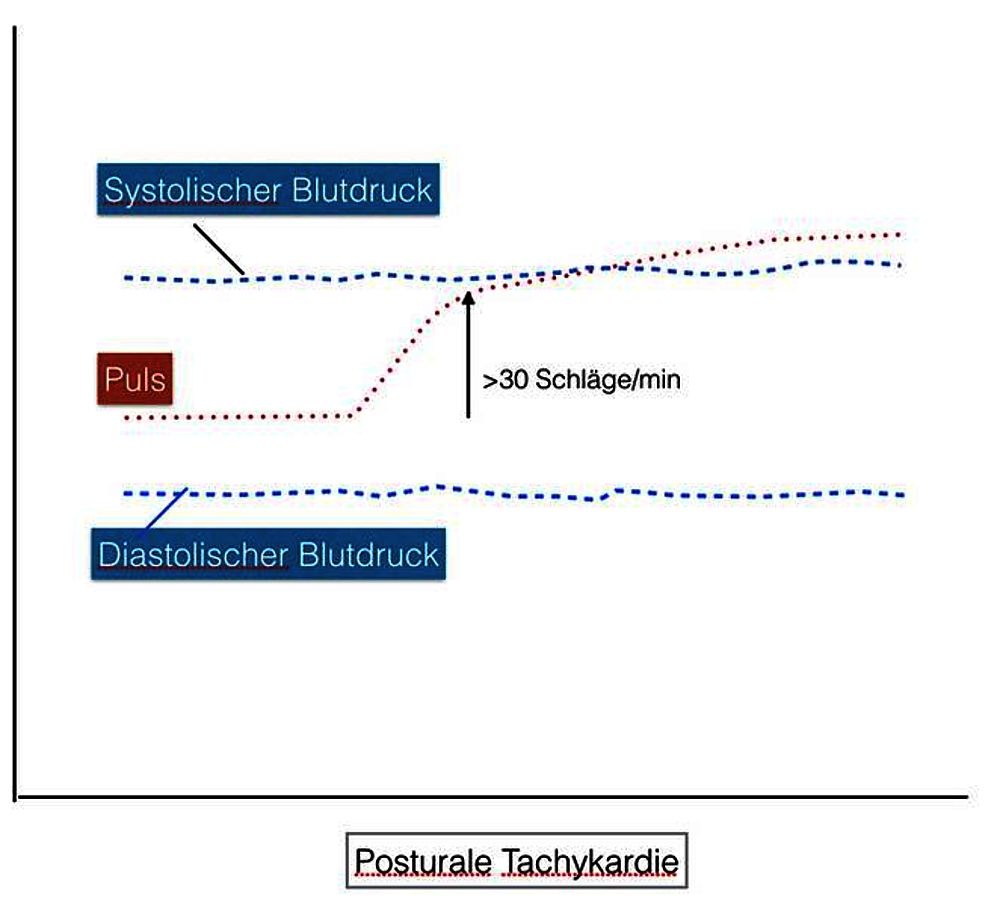
In postural tachycardia, sufferers feel most comfortable when lying down. But woe betide you when you stand up. Then the pulse suddenly jumps up by 30 or more beats per minute.
But that's not all: there is a feeling of emptiness in the head, nausea, weakness, trembling, anxiety and sometimes feelings of panic. After a while, above all, a barely controllable exhaustion sets in.
Some lie down almost the whole day and are hardly able to lead a normal everyday life.
It is about backgrounds, causes and therapy possibilities.
New: Our POTS APP
Introduction
Symptomatology
What is postural tachycardia syndrome (POTS)?
A POTS is defined as an abnormal circulatory regulation in which.
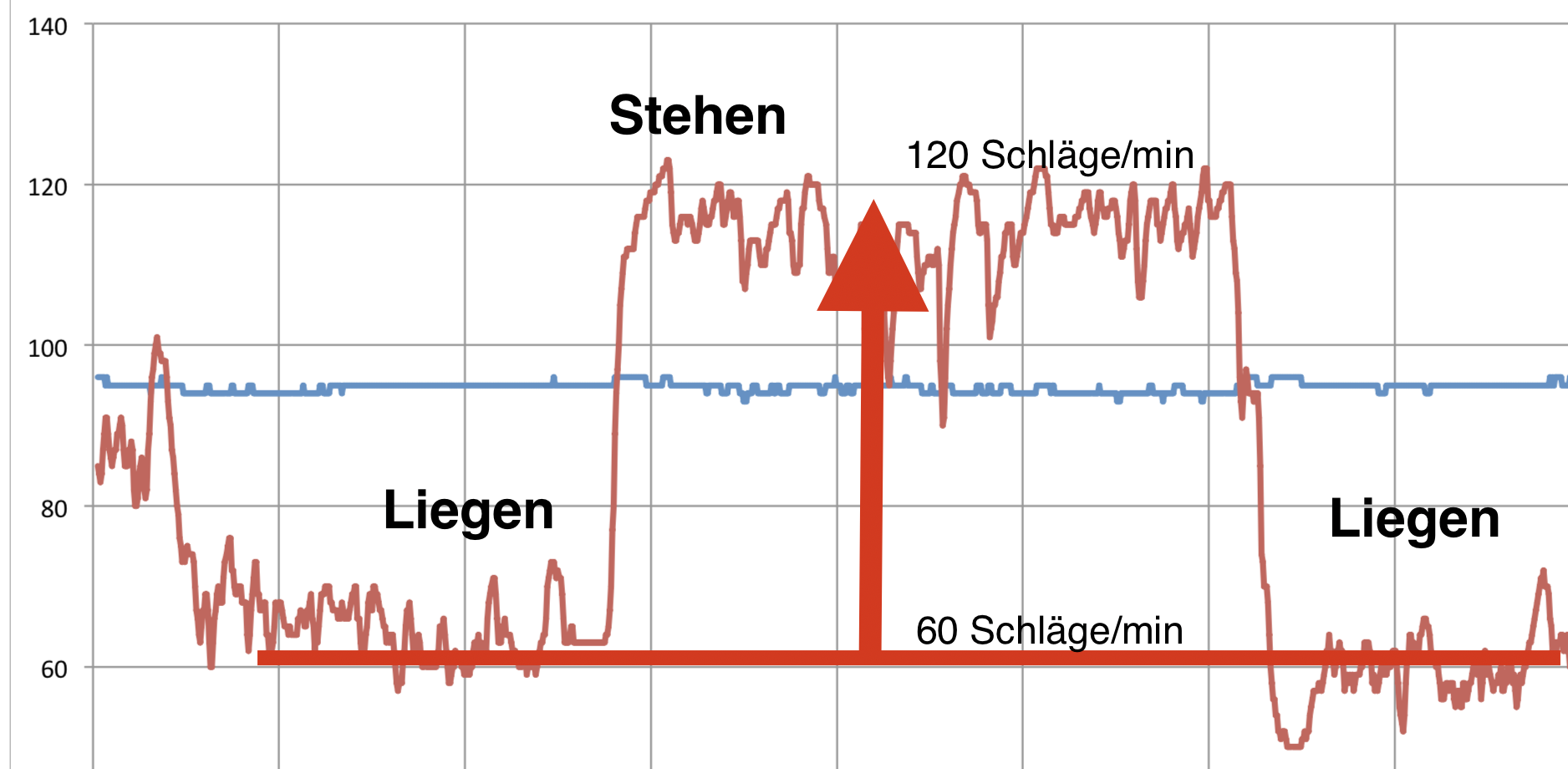
- Either the heart rate increases either by at least 30 beats/minute or to at least 120 beats within 10 minutes of standing.
- Blood pressure is largely unchanged (systolic does not drop more than 20 mmHg, diastolic does not drop more than 10 mmHg)
- Complaints occur (dizziness, lightheadedness, etc.)
- No other explanatory disease is present
(In adolescents (12-19), a rate increase of 40 beats is required for diagnosis).
Historical
The symptomatology was first described in the mid-19th century as "soldier's heart" or "irritable heart" byDaCosta. Other names were "mild orthostatic intolerance," mitral valve prolapse, neurocirculatory asthenia, or psychiatric diagnoses were given.
The current definition dates from 1993.
Complaints
Mostly, those affected complain of empty or "absorbent cotton" feelings in the head, drowsiness, unsteadiness when standing, dizziness, palpitations, nausea, trembling, weakness, shaking, standing becomes difficult and they have the desire to sit down again.
In the course of the disease, which often lasts years, there is very often increasing and sometimes massive exhaustion. Many of those affected lie down a lot during the day and are hardly able to organize a normal daily routine.
There are smooth transitions to CFS and other exhaustion syndromes.
Frequency
The frequency of the disease is not completely certain, probably a few per thousand to one percent of the population are affected. Especially young women or women before menopause are basically affected about 4-5 times as often as men. Mostly the symptomatology starts under 18 years of age. There are indications that the symptomatology is increasing. However, this may also be due to increased awareness of the symptoms by physicians.
Many of them also suffer from other functional disorders as described on these pages, e.g. migraine, irritablebowel symptoms,irritable bladder symptoms,pain disorders,exhaustion syndromes,sleep disorders,dizziness, the feeling of being "packed in absorbent cotton" or nausea. In the psychological field,anxiety disorders and depression are common.
Severely affected
POTS can lead with very high impairment up to permanent bed confinement and disability. About 25% are permanently unable to work and then usually suffer additionally from depressive symptoms, anxiety and numerous vegetative complaints. The overlap withchronic fatigue syndrome (CFS)is particularly striking.
After 5 years, in onestudy, the symptomatology was improved in 50%. However, 81% did not remain fully recovered!
Much unclear
The cause of POTS is not yet fully understood. As with most functional disorders, women are affected far more often (about 80%) than men. Again, it seems to be the sensitive, rather more anxious younger women who suffer from the symptomatology more often. It is possible that very feminine women with soft, stretchy connective tissues who are also otherwise prone to edema (water retention) are more often affected.
Anxiety and hyperventilation appear to be major factors leading to chronicity.
Especially with long duration, loss of fitness, sparing, and general withdrawal are likely to contribute in many ways to further deterioration.
Diagnosis
Diagnosis
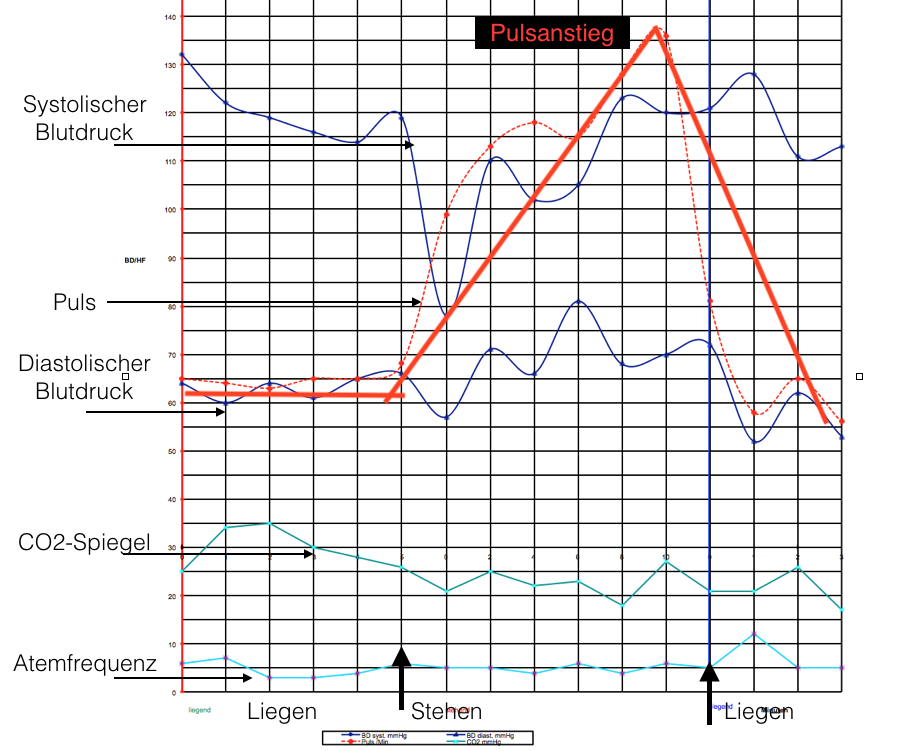
The diagnosis of postural tachycardia syndrome is usually performed using a tilt table. After a period of lying down (10 minutes), the patient is then raised to about 80°. Over the course of 10 minutes, there should then be a pulse increase above 30 beats per minute (or >120) without much change in blood pressure.
Without a tilt table, the test can also be performed as a so-called "Schellong test". Here, too, the patient first lies down and then stands up.
Of course, it is essential that other causes are excluded, such as certain medications (e.g. diuretics), heart disease or similar.
Subforms
(copy 9)
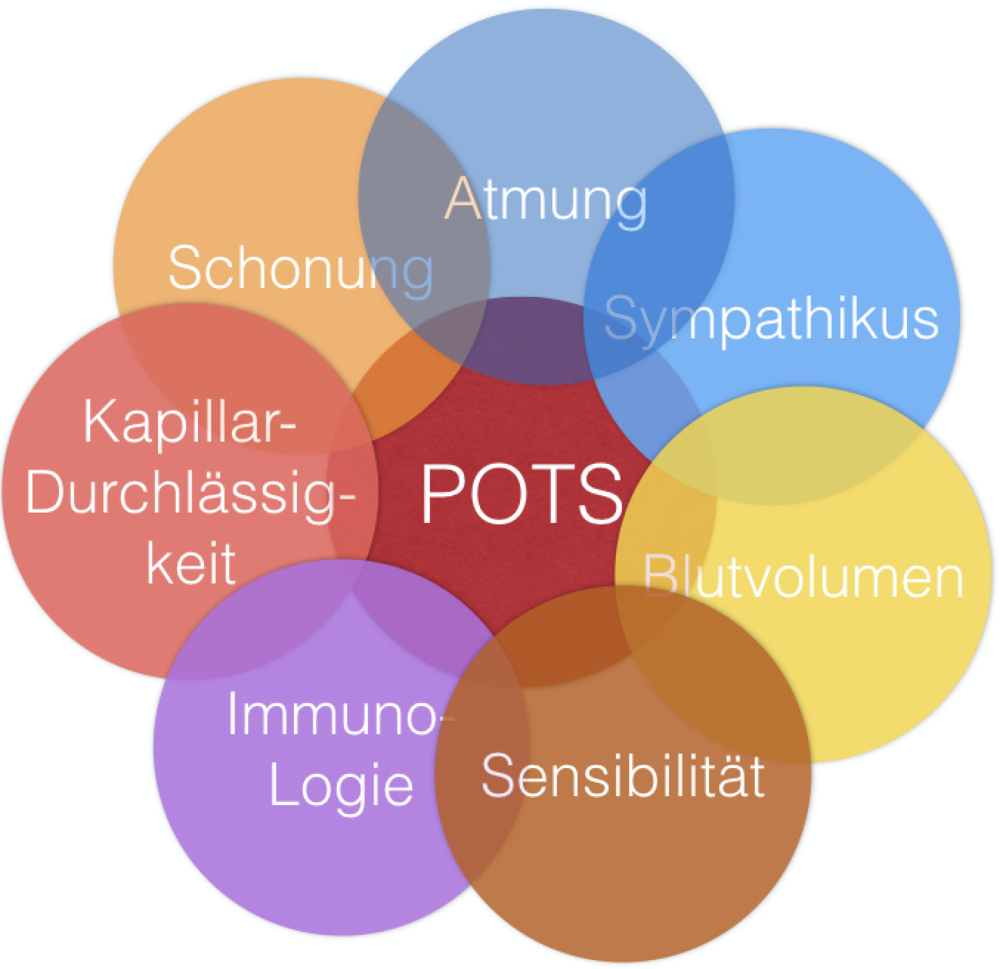
POTS is a multiform clinical picture, which can arise from different causes and it is so far also is understood only to a small part.
Here is a possible classification:
Neuropathic - impairment of the nerves
At least in some patients, there is apparently damage to the nerves in the legs. This leads to a reduced contraction of the veins and the blood remains "stuck" in the legs. This often results in a disturbance of the sweat secretion of the feet.
However, this finding is qualified: some affected persons also have an increased sympathetic activity, which may be explained reactively. In this case, other signs of sympathetic activity are also found: sweating, palpitations, inner restlessness.
Hypovolemic - lack of fluid
In about half of the patients, a reduced blood volume is found - which can be reduced by up to one liter (!). Standing up may cause a critical point to be exceeded where there is simply too little blood circulating.
Here, the control of the kidneys may be impaired. Findings of altered renin and aldosterone concentrations point in this direction.
Adrenergic- enhanced sympathetic activity
About half of the patients show signs of increased sympathetic activity. They suffer more from palpitations, palpitations, anxiety, restlessness, sweating or trembling. Their systolic blood pressure may be elevated.
Hyperventilatory - breathing too fast
There is a clear clustering of POTS and hyperventilation according to theliterature and our own observations.
Accelerated breathing leads to a drop in the CO2 level (so-called hypocapnia). This causes, among other things, anarrowing of the arteries of the cerebral vessels. This leads to a reduced blood supply to the brain and is likely to explain a large part of the central symptoms(exhaustion,dizziness, lightheadedness, visual disturbances).
This also opens up new therapeutic possibilities, which go beyond influencing the breathing. See our pages onhyperventilation.
Connective tissue related - overstretchable connective tissue
Here, a very stretchable connective tissue is found, which mainly presents as hyperextensible joints. This is particularly pronounced inEhlers-Danlos syndrome, which is associated with highly stretchable skin and joints. In this disorder, up to 80% may present with POTS symptoms.
Immunological - antibodies against itself
In another part of the patient, increased activities of mast cells (so-called mast cell activation syndrome) are found, which also play a role in allergies. Various autoantibodies have been found here.
Likewise, there is POTS after vaccinations or - similar toCFS- after severe infections. These could be up to 50% of those affected.
Causes
(copy 11)
Different hypotheses
The disease is still only partially understood. Numerous aspects seem to play a role, which are also mixed to varying degrees. As with most functional disorders, women are affected far more often (about 80%) than men. In turn, it seems to be the sensitive, somewhat more anxious younger women who suffer from the symptomatology more often.
As mentioned, the body regulates blood pressure upon rising with three mechanisms: venous and arterial vasoconstriction and increase in heart rate. In POTS, the first two are absent and blood pressure must be maintained only by the increased heart rate, which logically must then increase particularly dramatically. As also shown with the "subtypes", different parts of the regulation can be affected in each case.
Here are some of the causes that are often found in POTS.
Stress and breathing
According to our own experience, stress usually plays a major role in addition to the known triggers (e.g. infections). The symptoms usually develop during or after stressful phases of life. Breathing is a very important factor. The majority of patients who have been treated by us also suffer from more or less pronouncedchronic hyperventilation.
Lack of volume
- In healthy persons, the blood volume decreases by approx. 300 ml after 3 minutes when standing, and by approx. 600 ml after 10 minutes, after which there is no further decrease.
- In POTS, this volume is doubled!
- The baroreceptors register the lack of volume and try to stabilize the circulation by accelerating the heartbeat.
Sympathetic nervous system
- Sympathetic fibers for vasoconstriction in the legs are impaired, or the release of adrenaline is decreased: Hypoadrenergic.
- A subgroup has a centrally increased sympathetic activity at rest with trembling, sweating, restlessness.
Baroreceptors - Pressure regulator
Humans have sensors that can determine the pressure in the bloodstream (baroreceptors or baroceptors). They are located especially in the carotid artery (carotin) and the aorta (aorta). There are studies that have found a normal response of the baroceptors when lying down but a particularly sensitive response when standing.
Blood volume
Reduced blood volume
- POTS patients have about 1 liter less blood volume (77-89%).
- Critical limit reached by standing (additional approx. 500 ml further loss).
Irritable bowel
Reid bowel symptomatology is more often found in POTS, asstudies and our own experience show. Irritable bowel syndrome could aggravate POTS because there is more blood in the bowel, which is then missing during the return flow to the heart during standing (venous pooling).
Increased permeability of the capillaries
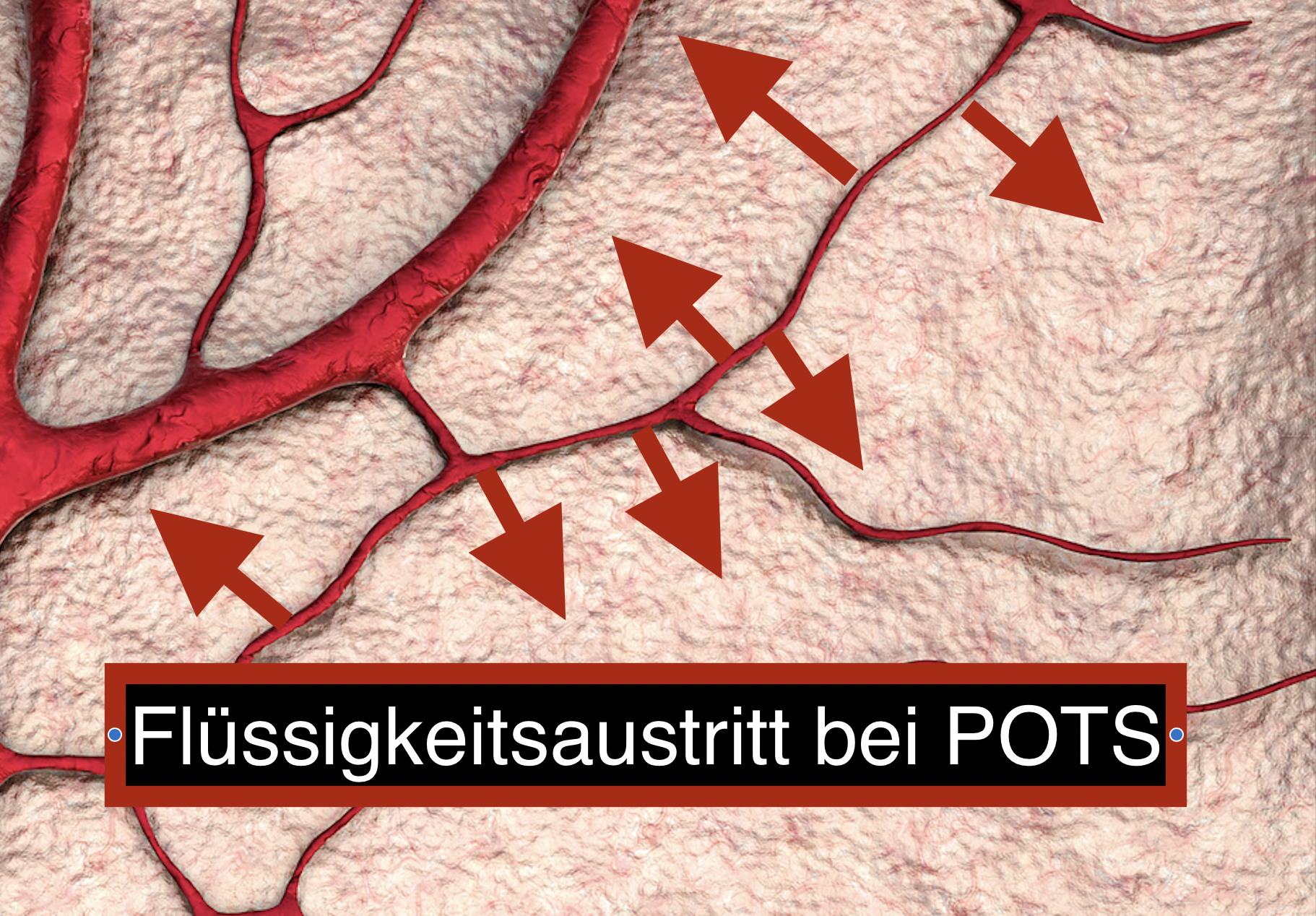
In some cases of POTS, the capillaries of the legs appear to leak increased fluid into the connective tissue. The longer the affected person stands, the more fluid is lost in the tissue.
This could explain why in healthy individuals the counter-regulation is completed after 1-2 minutes at the latest when standing up, whereas in POTS this is absent. They constantly lose more and more fluid into the tissues of the legs.
Mast cells
- Increased mast tent activation in a proportion of POST patients.
- Indications: Flash, nausea, vomiting, hyperadrenergic reactions with palpitations, hypertension.
Protection
Long periods of inactivity and rest lead to a reduction in the stroke volume of the heart and a decrease in blood volume. However, this is also the case with prolonged bed rest.
This aspect seems to us to be very relevant in prolonged POTS.
Autoimmune processes
An autoimmune process is triggered after a viral infection. It seems important to note that many autoimmune processes affect women of childbearing age.
Reduced blood flow to the brain

A very substantial part of the symptomatology seems to be explained by a reduction in Hindruch's blood flow.
Briefly, it is about the following relationship. If one breathes too fast while standing, there is a drop in the CO2 content of the blood. This, in turn, causes disfiguration of the vessels of the brain with reduced blood flow.
Studies have shown the following:
- When standing, there is a significant restriction in cerebral blood flow (20% vs. 10% in healthy individuals).
- This correlates directly with hypocapnia (CO2 decrease) and hyperventilation.
- In healthy individuals, drop in standing by 4 mmHg in POTS by 10 mmHg.
- Anxiety/panic correlates with hypocapnia/hyperventilation and acts as a reinforcing mechanism
- More details also here.
Concomitant diseases
Concomitant diseases
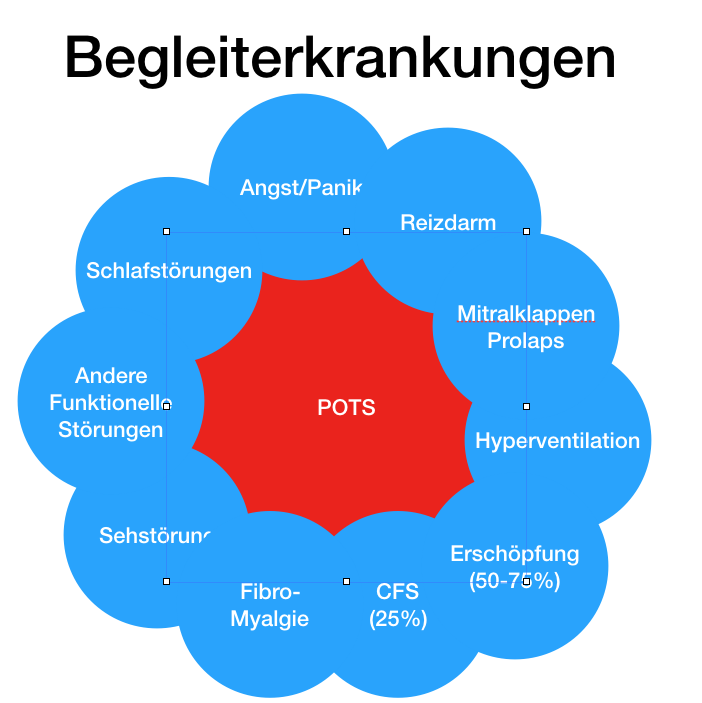
POTS rarely or never occurs alone. Usually numerous other so-called functional disorders are associated with it, which also gives an indication of the cause of the symptomatology. The basic considerations and the respective clinical pictures can also be found on these pages. The following complaints are particularly common:
- Anxiety disorders/panic disorder (however, the tachycardia is not caused by anxiety but by standing up!)
- Irritable bowel syndrome
- Irritable bladder
- Mitral valve prolapse
- Disturbance of sweat secretion
- Fatigue syndromes (approx. 50-75%)
- CFS (approx. 25%)
- Fibromyalgia
- Sleep disorders (lack of rest, daytime sleepiness)
- Pressure sensations in the thorax
- Visual disturbances
- Hyperventilation
Irritable Bowel Syndrome
In POTS, irritable bowel symptoms are also very frequently found. In our experience, this is the rule rather than the exception and similar indications can be found in the literature.
Increased venous pooling (i.e., more blood) in the abdomen may play a role, whereby return flow to the heart may be impaired.
Prolonged passage time, activation of mast cells in the gut, and general hypervigilance to bodily processes may also play a role in irritable bowel syndrome.
Vascular compression
Compression syndromes of the vessels are frequently found:
- Thoracic outlet syndrome
- Truncus coeliacus compression syndrome
- Pelvic congestion syndrome
Other diseases
- 50% acrocyanosis - livid (blue), cool legs/hands/feet
- Livedo reticularis
- Eczema
- Raynaud's syndrome
- Ehlers-Danlos syndrome in 18% and hypermobility of joints
Posturale Hyperventilation
Little noticed: Breathing while standing!
In some patients with POTS, not only the pulse reacts with an acceleration, but also the breathing. Those affected breathe faster and, above all, more deeply.
This reaction had escaped us for a long time, but it has decisive consequences for the complaints.
At first glance, the behavior may seem strange. Why should someone breathe differently when standing? But there is a deeper physiological meaning behind it. Namely, the increased diaphragmatic activity ends up transporting more blood toward the brain. It works like this:
With each upward movement of the diaphragm, it draws blood from the leg veins.
When it moves downward, it would be forced back into the legs if it weren't for the venous valves preventing it from doing so.
Thus, during inhalation (diaphragm downward), the pressure in the abdomen increases and the blood is transported through the diaphragm into the chest cavity and thus to the heart.
Breathing - To stabilize the circulation
In POTS, this mechanism - which is completely normal at its core - has a special significance. Since the normal response to standing (the activation of the veins) is impaired, the pulse must be increased as a substitute and the diaphragm must also be activated to help stabilize the circulation.
Increased, deep breathing thus transports more blood upward from the veins toward the heart and brain.
Small blemish: drop of carbon dioxide
But this deepened breathing unfortunately also has an undesirable side effect. Although maximum oxygen is absorbed (100% saturation in the above example), the level of carbon dioxide drops at the same time, since more is exhaled.
Central office impairment
We therefore strongly suspect that the numerous "central symptoms" - symptoms of the brain - are explained by this mechanism.
- Absorbent cotton feelings
- Concentration problems
- Head pressure
- Exhaustion
- Visual disturbances
- Drowsiness
- Feeling of anxiety
- Anxiety/Panic
Therapy: Multimodal
First of all disappointing!
If you are looking for a simple treatment for POTS and postural hyperventilation, you will be disappointed at first. There is not a single drug that has been approved for this purpose. Nor is it the case with the other procedures that a single measure is sufficient to successfully treat the complex symptomatology.
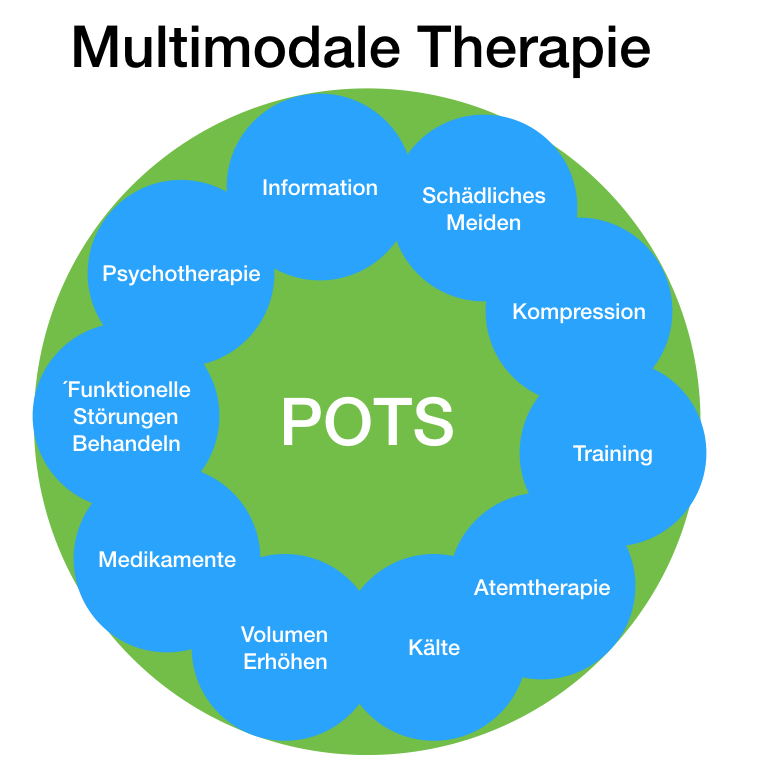
Instead, multimodal therapy is recommended, using a variety of procedures. How we treat the problem is presented here.
Module 1: Information
First of all, those affected need clear information about the background. Myths (amalgam poisoning, Lyme disease, cell phone radiation, etc.) do not help. The symptoms are also not a hidden message from the body, which wants to convey "through the flower" that "everything is too much". Psychological factors are important, but not the sole cause. There is now enough research and experience about the symptoms.
Everything that reduces anxiety and promotes relaxation is helpful.
Module 2: Harmful avoidance
One of the most important steps is to avoid anything unnecessary or harmful that may favor the course of the disease. This includes above all:
- Gentleness/Inactivity!
- Hyperventilation
- Excess weight
- Diuretics
- Calcium channel blockers
- Mineralocorticoid antagonists
- Beta-blockers (possibly unproblematic in some cases)
Module 3: Compression
In POTS, blood "pools" in the abdomen and legs (especially in the veins). Therefore, it is obvious to counteract this with external compression. There is also evidence in thescientific literature for this therapy, which we generally use.
In the above experiment you can see how directly effective this is.
- Compression stockings
- Compression tights
- Wrapping of the legs
- Compression of the abdominal area (by means of aids or also by muscle building)
- Various decongestive measures (lymphatic drainage, apparative compression, methods of skin tightening) as described on the pages on lipedema therapy.
- Circumference reduction of the legs - if necessary
Module 4: Training
When exhausted patients who spend most of the day lying down hear about "exercise," they just wave it off in resignation: it won't work at all! The more they force themselves, the worse they feel. Of course, this is logical: if too little blood reaches the brain, fatigue increases while standing.
In fact, theliterature shows that of all things, unpleasant exercise can bring significant improvements.
The "workout" must therefore be done initially without this negative effect on blood flow. That means: with gravity eliminated. About:
- Exercises while lying down (e.g., with rubber bands).
- Swimming
- Bed bike
We have therefore developed a first app that you can use to exercise at home. #
AlterG - cheat gravity!
POTS patients also learn to walk or even jog again with us! But for this we have a tricky aid. We use a treadmill that is wrapped up to the hips/chest. Air is now blown into this envelope, creating an overpressure that lifts the body. This creates the feeling of weightlessness or "seven-mile boots." At the same time, the veins of the abdomen/legs are compressed, thus eliminating the POTS problem.
The name AlterG is explained like this: "to alter" = to change. In physics, the letter "G" stands for the force of gravity. Of course, gravity is not changed - but the perceptible weight is.
Module 5: Breathing therapy
Especially if the pulse increase is coupled with hyperventilation, respiratory therapy becomes a central component of the measures.
You will find agreat deal of information on respiratory therapy on these pages. We have even created an online program for this purpose.
Module 6: Cold
The higher the temperature, the more there is an increase in venous filling of the legs. This can mean a third or more of additional filling in the heat.
This effect can be used! If the legs are colder (Kneipp, water, shorts) the symptoms are dampened.
We use this effect when walking and jogging in the cold chamber, where it is about -80° C. Sounds bad, but it is not. In this "cool" environment, for many POTS patients the symptoms are blown away.
Module 7: Increase volume
In POTS, blood volume is reduced in everyday life but also acutely when standing. Therefore, it is useful to replenish the circulation:
- Increase blood volume: Drink 2.5-3 liters
- Add common salt: e.g. high-salt diet, salt tablets
- Infusion of NaCl: 1 liter within 1-2 hours
Module 8: Medication
There is no single approved drug against POTS! Therefore, taking them is usually more of a trial than a causal therapy. Our own experiences with the preparations are rather sobering. Therefore, drug therapy is rather the exception with us. Nevertheless, medication may be indicated in individual cases.
Of course, the following always applies: Discuss all measures with your doctor. Do not take anything without a prescription. Things can also get worse.
- Administration of alpha1-agonists: Enhancement of the sympathetic effect: Midodrin - Gutron®
- Beta-blockers in very low dosage against panic feelings in tachycardia (worsen exhaustion)
- Anti-allergics (for mast cell activation)
- Mineralocoricoids: Antonin H 0.1mg (1-2 x daily)
- Desmopressin, Minirin® as tablets (antidiuretic)
Resist the temptation to rely only on medications!
Module 9: Treatment of concomitant symptoms and diseases
POTS practically never occurs in isolation. As a rule, it is accompanied by otherfunctional complaints. There is an intensive interaction and mutual reinforcement between these different symptoms. If, for example, there are pain symptoms or irritable bowel complaints, these should definitely be treated as well. More about this in the individual clinical pictures on this page.
Module 10: Psychotherapy
The soul also has a strong influence on POTS. Especially anxiety, panic and depression as well as inner "catastrophizing" often make the complaints worse. Therefore, accompanying psychotherapy is useful and often part of our therapy.
However: Psychotherapy as asole measure isnot sufficient. It should always take place within the framework of a multimodal therapy.
Multimodal therapyei g
POTS is a complex problem in which many aspects are intertwined. Especially when severe exhaustion is added to the pure circulatory disorder, isolated measures are often no longer effective. In this case, extensive therapies are necessary. As a rule of thumb, the most difficult thing to do should be practiced.
We could determine that therapies in larger time intervals (once, twice a week) are not able to change the profound misregulation. Therefore, we treat as intensively and comprehensively as possible over shorter periods of time. Often, patients come to us for two weeks and then continue to practice what they have learned at home.
The intensity also depends on the current resilience. If this is low, breaks in the course of the day are appropriate.
If the capacity is low, intermittent therapy sequences (e.g. several times a week) are more suitable. In between, intensive self-help takes place at home, which we supervise online if necessary.